International Journal of Anatomical Sciences 2010, 1: 21-25
Research Paper
A Study of the Anatomical Variations of the Circle of Willis Using Magnetic Resonance Imaging.
Haripriya M, Melani RS.
Department of Anatomy, Sri Ramachandra Medical College & Research Institute, Sri Ramachandra University, Chennai, India.
Key Words: circle of Willis, magnetic resonance imaging angiography, anastomosis
Abstract: Variations in the circle of Willis was studied using Magnetic Resonance Imaging Angiography in fifty patients of South Indian population at random. Variations have been found in 16 cases. All arteries in the circle of Willis showed variations except the anterior communicating artery, 5 cases showed variations in the anterior cerebral artery, 6 cases in the internal carotid artery, 2 cases in the posterior cerebral artery, 1 case in the posterior communicating artery and 2 cases in the basilar artery. Magnetic Resonance Imaging is the best tool to show the collateral circulation and the anastomotic variants of the circle of Willis.
Circle of Willis is a large arterial ring which unites the internal carotid and vertebro-basilar systems. It is formed of an anastomosis between the internal carotid artery, anterior cerebral artery, anterior communicating artery, posterior communicating artery and posterior cerebral artery (Williams et al., 1995). The anastomosis thus provided by this vascular ring is of great significance when one of the major arteries supplying the brain becomes occluded. The neurological deficit suffered as well as the ability of a patient to withstand occlusion of one or more of these major vessels depend on the presence of collateral circulation to the affected area. The haemodynamics of the circle is influenced by the variations in the caliber of communicating arteries and in the segments of the anterior and posterior cerebral arteries which lie between their origins and their junctions with the corresponding communicating arteries. A detailed know- ledge of the normal anatomy of the circle of Willis, its anomalies, and the clinical significance of its variations is valuable to the clinicians and neuroradiologists. Therefore this study was carried out to find out the variations of the circle of Willis using Magnetic Resonance Imaging Angiography.
Correspondance to: Haripriya M, Department of Anatomy, SRMC & RI, Sri Ramachandra University Chennai- 600 116, India.
Email: [email protected]
Materials and Methods
Fifty patients at random from the Out Patient Department of Radiology and Imaging Sciences, Sri Ramachandra Medical College and Research Institute, Sri Ramachandra University for undergoing MRI were chosen for the study. The technique used was three Dimensional Time of Flight Magnetic Resonance Angiography (3D-TOF-MRA). Only the arteries forming the circle of Willis were studied. For the purpose of identification,the circle of Willis is divided into anterior and posterior configurations.The anterior configuration consisting of the anterior cerebral artery,anterior communicating artery and internal carotid artery. The posterior configuration consisting of posterior cerebral artery, posterior communicating artery and basilar artery. For the purpose of description,the segments of the anterior and posterior cerebral arteries are named as :
1. Anterior cerebral artery – horizontal (A1) segment that extends medially from its origin to its junction with the anterior communicating artery.
2. Posterior cerebral artery – Pre- communicating (P1) segment extends laterally from its origin at the basilar bifurcation to its junction with the posterior communicating artery.
Observations
Out of the fifty cases, only sixteen cases showed variations of the circle of Willis whereas others were found to be normal (Fig. 1).
Fig. 1 showing normal circle of Willis
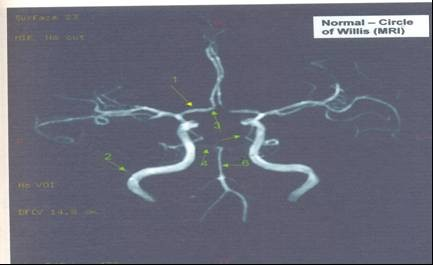
1. anterior cerebral artery
2. internal carotid artery
3.anterior communicating artery
4.posterior cerebral artery
5.posterior communicating artery
6.basilar artery
The findings were:
1. Hypoplasia of the A1 segment of the right anterior cerebral artery in 5 cases (Fig. 2).
2. Hypoplasia of left internal carotid artery in one case (Fig. 3) and stenosis in 5 cases on the right or left sides (Fig 4).
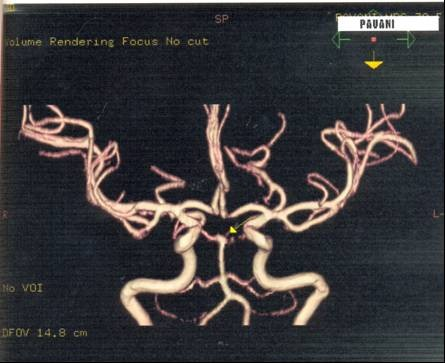
3. Hypoplasia of P1 segment of the right posterior cerebral artery in one case (Fig. 5) and diffused narrowing on the right side in another case (Fig. 6).
4. Absence of right posterior communicating artery and hypoplasia of left posterior communicating artery in the same case.(Fig. 7).
5. Stenosis of basilar artery in one case (Fig. 8) and ectactic changes in another case (Fig. 9).
6. No changes were observed in the anterior communicating artery.
Fig. 2 showing hypoplasia of the A1 segment of the right anterior cerebral artery.
|

Arrow indicates hypoplasia
Fig. 3 showing hypoplasia of left internal carotid artery
|

Fig. 4 showing tight stenosis of right internal carotid artery
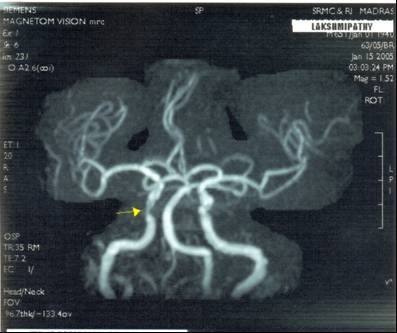
Fig. 5 showing hypoplasia of right posterior cerebral artery
|

Fig. 6 showing diffuse narrowing of right posterior cerebral artery

Fig. 7 showing absence of right posterior communicating artery and hypoplasia of right posterior communicating artery
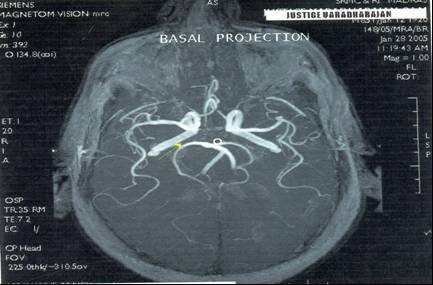
Fig.8 showing stenosis of basilar arteryFig.

9 showing bulbosity of basilar artery
Discussion
Variations of the circle of Willis have been studied by many investigators. Al-Hussain et al (2001) carried out a study to describe the main variations of the circle of Willis to clarify the clinical importance of these variations. In his study, out of 50, only 14 polygonal types of circle of Willis were observed; whereas in the present study of 50 cases 16 cases showed variations in the circle of Willis.
In a study by Macchi et al (2002) by MRA, the variability of the circle of Willis in 118 persons showed normal circle of Willis in 47%, complete anterior configuration in 90% and complete posterior configuration in 48.5%. Voljevica et al., (2004) analyzed angiographies of 150
MRI patients, in which a complete anterior configuration of the circle of Willis was seen in 76% with hypoplasia of the anterior cerebral artery. But in the present study, normal circle of Willis was 46 % with hypoplasia of anterior cerebral artery, complete anterior configuration was 78% and complete posterior configuration was 90%. Circle of Willis is regarded as the major source of collateral flow in patients with severe carotid artery disease (Hendrikse et at., 2001).When planning carotid surgery the configuration of the circle of Willis should also be taken into account. The cost of treatment of ischaemic stroke is increasing. Carotid bifurcation surgery can change the prognosis for symptomatic patients with over 70% of cartotid narrowing. Explanation of the carotid bifurcation is an important step in the diagnosis and must assess the degree of stenosis, the smoothness of the plaque and the collateral vessels (Rolland et al., 1996).
In the observations of Szabok et al. (2001), statistical analysis showed a significant relationship between the degree of stenosis and observed stroke pattern. In the present study of 50 patients, high grade internal carotid artery stenosis was seen in 10%. Although in the individual patient, any of the infarct patterns may occur, in statistical terms the incidence of a particular stroke pattern is clearly dependent on the degree of stenosis. Therefore territorial stroke can occur in internal carotid artery stenosis. The present study also showed absence of posterior communicating artery on the right side and hypoplastic posterior
communicating artery on the left side and the internal carotid arteries on either side appeared normal in its course and caliber. But the patient had lacunes in both cerebral hemispheres. In a similar study by Schomer et al., (1994), it was concluded that absent ipsilateral posterior communicating artery is a risk factor for ischaemic cerebral infarction in patients with internal carotid artery occlusion.
A small or absent ipsilateral posterior communicating artery is a risk factor for ischaemic cerebral infarction in patients with internal carotid artery occlusion. De Felice et al., (2000) studied bilateral non functioning posterior communicating arteries of circle of Willis in idiopathic sudden hearing loss in some patients and suggested a strong association between a non-functioning posterior communicating artery of the circle of Willis in sudden hearing loss. After the occlusion of an internal carotid artery the principal source of collateral flow is through the arteries of the COW, but the size and patency of these arteries are quite variable. Study of the anatomy of the collateral pathways in patients with ICA occlusion with or without infarction in the watershed area of the deep white matter may identify patterns that afford protection from ischaemic infarction (Brunere et al., 1995).
|
In the present study in one case, the basilar artery showed ectactic change at its bifurcation. The basilar artery aneurysm can cause stroke which may be due to thrombosis of the perforating arteries, arterio-arterial emboli or a compressive mechanism. Since sub arachnoid haemorrhage secondary to rupture of a dolichoectasia is exceptional, some authors antiaggregation in patients with ischaemia, where dilatations are limited to the basilar artery (Arenas et al., 2001).
Conclusion
The signal intensity of blood flow within a vessel is dependent on the replenishment of fully magnetized spins at the entry of the imaging section. Accordingly, non-visualization of a vessel may be either due to the absence of the vessel or to a very slow or turbulent flow within the vessel itself. Completeness of the configuration of the circle of Willis evaluated by using 3D-TOF-MRA is thus expected to be under estimated, both in healthy subjects that may show a negligible flow across the communicating vessels due to the symmetrical blood supply to the circle of Willis and in patients with severe stenosis or occlusion of the internal carotid artery that may show turbulent flow in one or more segments of the circle of Willis due to the presence of collateral pathways
MRA for determining the degree of carotid stenosis prior to carotid endarterectomy is attractive because it does not have the high morbidity associated with conventional intra-arterial angiography. Both atherosclerotic and non-atherosclerotic carotid artery disease can be comprehensingly assessed with contrast enhanced Magnetic Resonance Angiography. Contemporary understanding of the collateral circulation may be greatly enhanced through further refinement of neuroimaging modalities that correlate angiographic findings with perfusion status, providing the basics for future therapeutic and prognostic applications.
Therefore it can be concluded that MRI is the most powerful non-invasive method to demonstrate collateral circulation via the basal communicating arteries and to identify haemodynamically relevant anatomic variants of the circle of Willis.
References
Al Hussein SM, Shoter AM and Bataina ZM (2001) Circle of Willis. Saudi Med J, 22: 895 – 898.
Arenas-Cabera C, Martinez-Fernandez E, Gil-peralta A, Sanchez-Huelva A, Cabrera-Perez R and Chinchon-Lara T (2001) Repeated strokes in a patient with a basilar artery aneurysm. Rev Neuro, 32: 335-338.
Brunereau L, Levy C, Bousson V, Marsot – Dupuch K, Bousser MG and Tubiana JM (1995). Anatomy of the Circle of Willis with 3D time of flight magnetic resonance angiography and analysis of partitions. J Radio, 76: 573 – 577.
De Felice C, De Capma B, Tassi R, Mencattini G Passali D (2000) Non-Functioning posterior communicating arteries of Circle of Willis in idiopathic sudden hearing loss. Lancet, 356:1237 – 1238.
Hendrikse J, Hartkamp MJ, Hillen B, Mali WP, Vander-Grond J (2001) Collateral ability of the Circle of Willis in patients with unilateral internal carotid artery occlusion, border zone infarcts and clinical symptoms. Stroke, 32: 2768– 2773.
Macchi C, Lova RM, Miniati B, Gulisano M, Pratesi C, Conti AA and Gensini GF (2002) The Circle of Willis in healthy older persons. J Cardiovasc Surg (Torino), 43: 887 – 890.
Rolland Y, Sirop V, Lucas A, Rambeau M, MOrcet N, Duraferrier R (1996) Multimodal approach to carotid bifurcation in atherosclerosis. Ann Radiol, 39: 221 – 233.
Schomer DF, Marks MP, Steinberg CK, Johnstone IM, Boothroyd DB, Ross MR, Pele NJ, Enzmann Dr (1994) The anatomy of the posterior communicating artery as a risk factor for ischaemic cerebral infarction. N Eng J Med,330: 1565-1570.
Szabok, Kern R, Gass A, Hirsch J, Hennerici M (2001) Acute stroke patterns in patients with internal carotid artery disease; a diffusion – weighted magnetic resonance imaging study. Stroke, 32:1323-1329.
Voljevica A, Kulenovic A, Kapur E, Talovic E, Vuckovic I, Luinovic A (2004) Presentations of variations in the anterior part of the Circle of Willis as a result of MRI- angiography method. Med Arh, 58: 327 – 330.
Williams PL, Bannister LH, Berry MM (1995)
Haemolymphoid System In: Gray’s Anatomy,38th Edition, Edinburgh and London: ELBS with Churchill Livingston. 1571-1574.