International Journal of Anatomical Sciences 2010, 1: 26-30
Research Paper
Morphology of the Intercondylar Notch and its Clinical Significance
Ravichandran D,a Melani R.b
Department of Anatomy, VMKV Medical College, Salem, Tamil Nadu, India; bDepartment of
Anatomy, SRMC &RI, Sri Ramachandra University, Chennai, Tamil Nadu, India.
Key Words: intercondylar notch, dimensions, anterior cruciate ligament
Abstract: The dimensions of the intercondylar notch of dry femora and in cadavers were measured and their clinical implications were assessed. The study was conducted in two groups, Group A (dry bones) and Group B (cadaveric knees). The dimensions including notch width, condylar width, notch depth, condylar depth and the shape of the notch were measured using standard guidelines in both groups. In group B, the status of the anterior cruciate ligament (ACL) was also noted and categorized. Using these datas, the notch width index (NWI) and notch depth index (NDI) were calculated. The results were analyzed statistically. The average notch width index was found to be 0.252 in dry bones and 0.230 in cadavers. The average notch depth index was found to be 0.467 in dry bones and 0.502 in cadavers. The shape of the notch (in both groups) in majority of the cases was “inverted U” and in few cases it was “triangular”. Sixteen knees showed laxity of ACL with marginal reduction of both indices. The clinical implications are discussed.
The shape of the intercondylar notch plays an important role in knee injuries. Triangular shaped notches with straight edges cause damage to the ligaments. The shape of the intercondylar notches were observed by many investigators (Anderson et al., 1987; Souryal and Freeman, 1993 and Shickendantz and Weiker 1993). The morphology of the intercondylar notch of the femur is related to the functioning of the cruciate ligaments. Abnormally narrow (stenotic) notches have been shown to increase the incidence of anterior cruciate ligament (ACL) injuries. The lower end of the femur presents two rounded and eccentrically curved condyles. The groove present anteriorly between them is called the patello-femoral groove. The notch separating them posteriorly is the intercondylar notch (Williams et al.,1995).The cruciate ligaments have intimate embryological and functional relationship to the intercondylar notch (Robert Miller,2008). The space available for the cruciate ligament is determined by the dimensions of the notch including the depth, width and shape.
Correspondance to: Ravichandran D, Department of Anatomy, VMKV Medical College, Salem 636 007
Tamil Nadu, India
Email: [email protected]
Narrowing of the intercondylar notch is termed as “intercondylar notch stenosis”. Few authors have noted a strong association between stenotic intercondylar notches and anterior cruciate ligament injuries (Souryal and Freeman 1993). The intercondylar notch is found to be significantly smaller in knees with severe osteoarthritis due to osteophyte growth in the notch (Wada et al., 1999), thus increasing the incidence of ACL ruptures in patients with degenerative arthritis (Heriberto Ojeda Leon et al., 2005). Literature regarding the morphology of the intercondylar notch in Indian population is scarce. Therefore an attempt has been made to determine these dimensions and their clinical implications in Indian population.
Materials and Methods
The study was conducted in two groups (A & B). Group A comprised of dry bone samples (n= 200 femora) and group B, cadaveric knees (n=40). Dry bones and cadaveric knees from the Departments of Anatomy, Vinayaka Missions Kirupananda Variyar Medical College, Salem and Sri Ramachandra Medical College & Research Institute, Sri Ramachandra University, Chennai were utilized for this study.
i) The dimensions of the femoral condyles and intercondylar notches were measured using a vernier caliper. In group A, the measurements were taken directly from the bones and in group B, the measurements were taken in the cadavers at the anterior outlet of the knees with the knee in 90 degrees flexion (Fig.1).
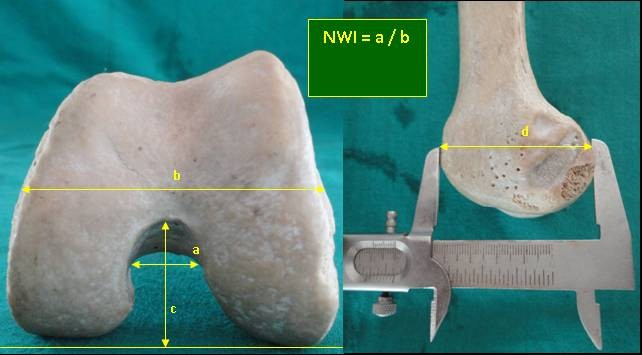
The measurements of the parameters were taken according to the guidelines given by Anderson et al., 1987; Herzog et al.,1994 and Wada et al., 1999. In both the groups, the notch width represented the width of the notch at two-thirds of the notch depth. The notch depth was identified as the maximum height of the intercondylar notch. The width of the femoral condyle between both epicondyles was measured as the condylar width and the maximum antero- posterior height of the lateral femoral condyle was measured (Wada et al., 1992) as the condylar depth (Fig. 2). The notch width index (NWI) and notch depth index (NDI) were calculated with these data. The shape of the intercondylar notches and the status of the ACL were also studied. The results were tabulated and analyzed statistically. The data of this study was analyzed using SPSS 15.0.
Fig 1 Measurement of notch width in cadaver with knee in 90o flexion
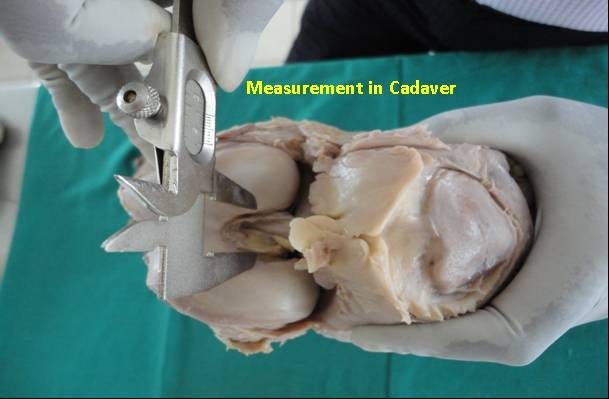
Fig 2 Measurement of different parameters (a – notch width b – condylar width c – notch depth d –condylar depth)
|
Observations
The Descriptive Statistics like N, percentage, range, mean & standard error of mean including the Inferential statistics like student’s t-test (Swan, 2005) with p – value of dry bone parameters and cadaver parameters are tabulated (Table 1). The mean + SE of NWI and NDI in group A was found to be 0.252 + 0.002 and 0.467 + 0.003 respectively. The mean NWI and NDI ingroup B was 0.231 + 0.003 and 0.503 + 0.013 respectively.
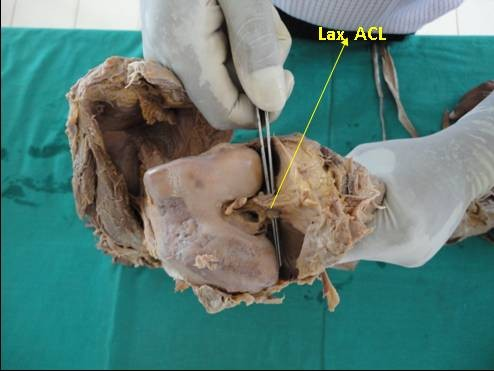
The shape of the notch in 67% of group A and 80% of group B was found to be “inverted U” and 33% of group A and 20% of group B showed triangular shaped notches (Fig. 3). 16 knees in group B showed laxity of ACL and 24 knees had normal ACL. A comparison of NWI and NDI between the knees with normal ACL and lax ACL showed a marginal reduction of both the indices in the knees with laxity of ACL ( 0.227 and 0.514 respectively).
Table 1. Descriptive & inferential statistics
| VARIABLE | N | SIDE | RANGE | MEAN | S E (MEAN) | 95% CI | T – value | P – value |
| GROUP ANotchWidthCondylar width
Notch Depth
Condylar depth |
200
200
200
200 |
Left (94) Right(106)Left( 94) Right (106)
Left (94) Right(106)
Left( 94) Right (106) |
12 to 269 to 2861 to 87
57 to 89
19 to 33 20 to 34
43 to 69 35 to 72 |
18.6518.8973.97
74.58
27.27 27.20
58.38 58.71 |
0.270.290.61
0.57
0.29 0.27
0.51 0.52 |
18.11 – 19.2018.31 – 19.4772.70 – 75.19
73.45 – 75.71
26.68 – 27.86 26.67 – 27.74
57.36 – 59.39 57.67 – 59.76 |
0.588
0.724
0.172
0.453 |
0.557
0.470
0.864
0.651 |
| GROUP BNotchWidthCondylar
Width
Notch Depth
Condylar depth |
40
40
40
40 |
Left ( 21) Right ( 19)Left ( 21) Right ( 19)
Left ( 21) Right ( 19)
Left ( 21) Right ( 19) |
14 to 2315 to 2265 to 88
66 to 94
21 to 37 24 to43
42 to 73 54 to 71 |
18.1419.0579.19
81.94
29.95 30.68
58.95 63.47 |
0.500.501.28
1.61
0.83 1.08
2.35 1.00 |
17.08 – 19.2017.98 – 20.1276.51 – 81.87
78.54 – 85.34
28.20 – 31.70 28.41 – 32.95
54.04 – 63.85 61.35 – 65.58 |
1.260
1.347
0.543
1.707 |
0.215
0.186
0.592
0.096 |
Fig. 3 Different shapes of the intercondylar notch noted in the present study

Fig.4 Shows lax ACL in one of the knees of Group B
Discussion
The ACL is one of the commonly injured ligaments in athletes and in patients with degenerative osteoarthritis. Orthopaedic surgeons describe the injuries of ACL as “the beginning of the end of the knee”. The exact incidence remains unknown (Robert Miller, 2008). The ACL courses approximately at an angle of 40 degrees from its tibial attachment to the femoral attachment. The roof of the intercondylar notch is inclined 40 degrees to the longitudinal axis of the femur so that when the knee is in full extension, the roof is near the anterior surface of the anterior cruciate ligament (Robert Miller, 2008). The morphology of the notch therefore plays a very important role in the injuries of ACL.
In this regard, notch width index (NWI) has frequently been used as an indicator of stenosis (NWI < 0.20) of the intercondylar notch (Anderson et al., 1987; Souryal and Freeman 1993; Shickendantz and Weiker, 1993). The NWI represents the ratio of the notch width to the condylar width of the femur. In his study on 902 high school athletes using tunnel view radiographs of the knee joint, Souryal and Freeman (1993) found the normal notch width index to be 0.231 + 0.044. In the present study a comparison of NWI and NDI between knees with normal ACL and lax ACL in group B, a marginal reduction of both the indices were noted in the knees with laxity of ACL. This difference was not found to be statistically significant (p= 0.605 and 0.804 respectively). Yet it indicates a mild degree stenosis and hence a dysfunctional (lax) ACL. Therefore this study is more in favour of the association between the notch stenosis and ACL damage and feel that critical stenotic notches (NWI<0.20) may predispose to ACL tears.
Souryal and Freeman (1993) also observed variations of the index between men and women. The index for males was found to be larger than women. Therefore the female population is at a higher risk for ACL injuries than men.
Notch depth index (NDI) has also been used by some authors to predict the stenosis of the intercondylar notch (Wada et al., 1999), who had calculated the NDI as a ratio of the notch depth to condylar depth.
Anderson et al., 1987 observed variations in the shape of the intercondylar notch. According to him the shape may be “inverted U”, triangular or wave shaped. A narrow, triangular notch with straight edges increases the incidence of ACL ruptures (Shepstone 2001). The results of the present study in terms of NWI and NDI vary marginally with the observations of other authors. The NWI in the present study in group A (0.252 + 0.002) is observed to be slightly higher than the average value (0.231 + 0.044) as observed by Souryal and Freeman, 1993. The NWI as observed in group B in the present study is same as that observed by Souryal and Freeman, 1993 (ie 0.231). The NDI in the present study in group A (0.467 + 0.003) and in group B (0.503 + 0.013) is almost similar to the observations of Wada et al.,(1999).
Controversy exists among different authors regarding the association between intercondylar notch stenosis and ACL injuries. Muneta et al., (1997) and Teitz et al., (1997) have proved that intercondyar notch stenosis is not a significant risk factor for ACL tears. However a strong association between the intercondylar notch stensois in degenerative arthritis of the knee and increased incidence of ACL damage has been confirmed by others (Wada et al., 1999; Heriberto Ojeda Leon et al., 2005).
Conclusion
This study throws light on the normal range of intercondylar notch width index and notch depth index in Indian population. The study also infers that stenotic notches may be a cause for dysfunctional ACL and in extreme cases may lead to tear of the same. Therefore this study would be of great help to Orthopaedic surgeons in predicting and preventing the ACL injuries in athletes and in patients with degenerative arthritis.
References
Anderson AF, Lipscomb AB, KJ, Lindahl KJ, Addlestone RB (1987) Analysis of the intrcondylat notch by computed tomography. Am J Sports Med, 21; 110 – 113.
Heriberto Ojeda L, Carlos Rodriguez Blanco E, Todd Guthrie B, Oscar Nordelo Martinez J (2005) Intercondylar notch stenosis in degenerative arthritis of the knee. Am J Sports Med, 21(3);294 – 302.
Herzog RJ, Silliman JF, Hutton K, Rodley WG, Steadman JR (1994). Measurements of the intercondylar notch by plain film radiography and magnetic resonance imaging. Am J Sports Med, 22; 204 – 210.
Muneta T, Takakuda K, Yamamoto H (1997).
Intercondylar notch width and its relation to the configuraton and cross-sectional area of the anterior cruciate ligament. A cadaveric knee study. Am J Sports Med, 25: 69-72.
Swan AV (2005) In: Statistical Method. NewYork : Oxford Universtiy Press. 677-697.
Miller RH (2008) Knee Injuries. In: Campbell’s Operative Orthopaedics. 11th Edition, Volume 3, Mosby: Elsevier. 2496–2450.
Schikendantz MS, Weiker GG (1993) The predictive value of radiographs in the evaluation of unilateral and bilateral anterior cruciate ligament injuries. Am J Sports Med, 21: 11-13.
Shepstone L, Rogers J, Kirwan JR, Silverman BW (2001) Shape of the intercondylar notch of the human femur: a comparison of osteoarthritic and non–osteoarthritic bones from a skeletal sample. Ann Rheum Dis, 60: 968 – 973.
Souryal TO and Freeman TR (1993) Intercondlyar notch size and anterior cruciate ligament injuries in athletes. A prospective study. Am J Sports Med, 21: 535 –539.
Teitz CC, Lind BK, Sacks BM (1997) Symmetry of the femoral notch width index. Am J Sports Med,25: 687 – 690.
Wada M, Tatsuo H, Baba H, Asamoto K and Nojyo Y (1999) Femoral intercondylar notch measurements in osteoarthritic knees. Rheumatology, 38: 554 – 558.
Williams PL, Bannister LH, Berry MM (1995) Femur In: Gray’s Anatomy, 38th Edition, Edinburgh and London: ELBS with Churchill Livingston. 680