International Journal of Anatomical Sciences 2010, 1: 45-47.
Case Report
Levator Glandulae Thyroideae with the absence of Pyramidal Lobe – A case report
Gunapriya R, Varsha S, Senthil Kumar B.
Department of Anatomy, Saveetha Medical College, Thandalam, Chennai 602 105, India
Key Words: levator glandulae thyroideae, pyramidal lobe, infrahyoid muscles, thyroglossal duct, ectopic thyroid
Abstract: Levator glandulae thyroideae is a fibromuscular band, if present is usually on the left side connecting the pyramidal lobe of thyroid gland and the hyoid bone. The presence of levator glandulae thyroideae and its anatomical variations gain importance, in the pathologies related to thyroid gland and their treatment modalities. Hence, this case has been presented here for such a clinical significance.
Musculus levator glandulae thyroideae is a fibrous or fibromuscular band that stretches from the pyramidal lobe or upper border of isthmus of thyroid gland, usually on the left side, to the body of the hyoid bone above. (Standring, 2006). Mori (1964) classified levator glandulae thyroideae into five types; a) Hyopyramidalis, b) Thyreopyramidalis, c) Thyreoglandularis, d) Hyoglandularis, and e) Tracheoglandularis based on 210 levators, that he observed. Levator glandulae thyroideae observed in the present study fits into thyreoglandularis type (origin– thyroid cartilage, insertion – sheath of thyroid gland). This structure is said to represent the detached part of infrahyoid muscles and may be innervated by a twig from ansa cervicalis (Ranganathan, 2002)
Case Report
During routine dissection of neck, in a male cadaver aged about 60 years, the presence of levator glandulae thyroideae was observed on the right side. It was dissected with utmost care to look for its attachments above and below and for its innervation. A thin band of muscular like tissue stretched from the upper border of isthmus of thyroid gland, to the lower border of the lamina of thyroid cartilage, on the right side (Fig. 1). Hence, according to Mori’s classification, the levator glandulae thyroideae in this case belongs to Thyreoglandularis type. It measured 1 cm in length and 0.6 cm in breadth. Careful dissection revealed that there was no pyramidal lobe and this band did not have innervation from any nerve and did not extend up to hyoid bone. The thyroid gland and other structures in the vicinity appeared normal
As this tissue appeared to be muscular, it was subjected to microscopic study. The tissue was dissected out from the cadaver and sectioned at four levels. The tissues were then processed, and stained by hematoxylin and eosin stain, as described by Culling (1974). The study revealed the presence of thyroid follicles lined by cuboidal epithelium, with moderate amount of colloid in their lumina and surrounding fibrous tissue, at the lower levels (Fig. 2) and only fibrous tissue in the section taken at the upper level (towards the thyroid cartilage).
| Fig. 1 Photograph of the thyroid gland with the levator glandulae thyroideae
|

| Fig. 2 Photomicrograph of levator glandulae levator glandulae thyroideae thyroideae showing thyroid follicles with colloid and fibrous tissue surrounding the follicles
|
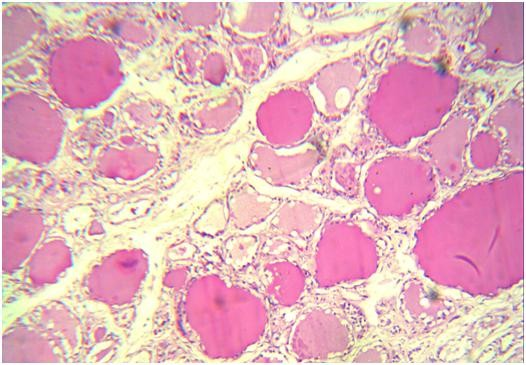
(TC-Thyroid cartilage; LGT-Levator glandulae (TF – Thyroid follicle with colloid; FT – Fibrous
Thyroideae; TG- Thyroid gland) tissue)
Discussion
Musculus levator glandulae thyroideae stretches from the pyramidal lobe or upper border of isthmus of thyroid, usually on the left side, to the body of the hyoid bone above (Standring, 2006). It may receive its innervation from external laryngeal nerve (Sinnatamby, 2007). Moore and Persaud (1999) have stated that pyramidal lobe is seen in 50% of population and the muscular band may be made up of smooth muscle fibres and that the pyramidal lobe and the associated smooth muscle represent the persistent part of distal end of thyroglossal duct. Another study done in 90 male cadavers revealed that, pyramidal lobe was present in 37.77%, frequently arising from the left lobe, while the levator glandulae thyroideae was present in 30% instances, mostly attached above to body of hyoid bone (Joshi et al., 2010).
The levator glandulae thyroideae observed in the present study is of thyreoglandularis type, which was found to be attached to thyroid cartilage on the right side, with no innervation from any nerve. The pyramidal lobe was also totally absent (Fig. 1). The microscopic study revealed that it was mainly made up of glandular tissue and partly by fibrous tissue towards the thyroid cartilage. Hence in this case, the levator glandulae thyroideae did not have innervation and it was made up of fibroglandular tissue (Fig. 2), which represents the persisting distal end of thyroglossal duct.
Accessory nodules / ectopic thyroid tissue of the thyroid are usually found at the embryonic origin of thyroid, at the foramen caecum and along the thyroglossal tract (Bergman et al., 2007; Ranade et al., 2008). Therefore the anterior cervical region has to be investigated very carefully during surgery, in order not to leave behind any residual thyroid tissue, during total thyroidectomy (Braun et al., 2007).
Conclusion
This study highlights the significance of thorough understanding of the thyroid anatomy and its associated anatomical variations, which thus form a cornerstone for safe and effective thyroid surgery.
References
Bergman RA, Afifi AK, Miyauchi R (2007) Thyroid gland In: Illustrated Encyclopedia of Human Anatomic Variation: Opus IV Organ Systems: Endocrine System (www.anatomyatlases.org/Anatomic variants/organ system/text/thyroidgland.html/)
Braun E, Windisch G, Wolf G, Hausleitner L, Anderhuber E (2007) The pyramidal lobe; clinical anatomy and its importance in thyroid surgery. Surg Radiol Anat, 29: 21-7.
Sinnatamby CS (2007) In: Last’s anatomy, regional and applied. 11th Edition, London : Elsevier – Churchill Livingstone. 352.
Culling CFA (1974) In: Handbook of histopathology and histochemical techniques. 3rd Edition, Great Britain: Butterworth and company. 211-214.
Joshi SD, Joshi SS, Daimi SR, Athavale SA (2010) The thyroid gland and its variations: a cadaveric study. Folia Morphologica, 69: 47-50.
Moore KL, Persaud TVN (1999) In: The developing human, clinically oriented embryology. 6th Edition, Singapore: A Harcourt Publishers International Company. 230.
Mori M (1964) Statistics on the musculature of the Japanese. Okajimas Folia Japan, 40: 195-300.
Ranade AV, Rai R, Pai MM, Nayak SR, Prakash, Krishnamurthy A, Narayana S (2008) Anatomical variations of the thyroid gland: possible surgical implications. Singapore Med J,49: 831-834.
Ranganathan TS (2002) In: A Textbook of Human Anatomy, 6th Edition, 497: New Delhi: S. Chand and Company Ltd.496-497.
Standring S (2006) In: Gray’s Anatomy, 39th Edition, London: Elsevier Churchill Livingstone. 561.