International Journal of Anatomical Sciences 2010, 1: 7-10
Research Paper
Diffuse Idiopathic Skeletal Hyperostosis
Ravichandran D, Muthukumaravel N,b Deepti S, Melani R, Subramaniam PM.
Department of Anatomy, VMKV Medical College, Salem, India; bDepartment of Anatomy, Annapoorna Medical College, Salem, India; cDepartment of Anatomy, SRMC&RI, Chennai, India; dDepartment of Pathology, VMKV Medical College, Salem, India
Key Words: thoracic vertebrae, anterior longitudinal ligament, supra-spinous ligament
Abstract: A dry bone specimen comprising six thoracic vertebrae held together by ossified anterior longitudinal and supra-spinous ligaments is reported. The specimen was subjected to plain radiography. The antero-posterior and lateral views confirmed the ossification of the above ligaments. Moreover, the ossified anterior ligament was found to be separated from the body of the vertebrae by a space and a radio-dense line paralleling the longitudinal axis of the vertebrae. The inter-vertebral disc space and the zygoapophyseal joint space were free. A piece of the ossified mass, subjected to histo-pathological examination also confirmed the ossified ligaments. Review of literature suggests that this is a case of diffuse idiopathic skeletal hyperostosis (DISH).
The anterior longitudinal ligament is extending from atlas to sacrum is a flat strong band found along the anterior surfaces of the vertebral bodies which becomes broader when traced caudally. It is thicker and narrower in the thoracic region than in the cervical and lumbar regions. The posterior longitudinal ligament on the posterior surfaces of the vertebral bodies inside the vertebral canal gradually narrows when traced downwards. These ligaments are adherent to the inter-vertebral discs, hyaline cartilage lining the articular surfaces, margins of adjacent vertebral bodies and the laminae. At various levels, ligamentous fibres blend with the subjacent periosteum, perichondrium and periphery of the annulus fibrosus (Williams et al., 1995).
Correspondance to: Ravichandran D, Department of Anatomy, VMKV Medical College, Salem, India. Email: [email protected]
Supraspinous ligament is a strongfibrous band connecting the tips of spinous process from C7 to the sacrum. Its most superficial fibers span over three or four spines, the deeper fibers bridge over two or three spines, while the deepest connect adjacent spines becoming continuous with interspinous ligaments (Williams et al.,1995). Heylings (1978) considers supra- spinous ligament to cease at the fifth lumbar spine.
The anterior longitudinal, posterior longitudinal and supraspinous ligaments (para-spinal ligaments) undergo degene- ration secondary to attrition, and they often ossify. This condition is broadly termed as spinal enthesopathy. Ossification involving the anterior longitudinal ligament is referred to as Forestier’s disease. Further, a diffuse variant exhibiting additional extra-axial features is termed as diffuse idiopathic skeletal hyperostosis (DISH)
Material and Methods
Morphological examination was undertaken on a dry bone specimen comprising six thoracic vertebrae held together by ossified anterior longitudinal and supraspinous ligaments, identified in the bone bank of the Dept. of Anatomy, VMKV Medical College, Salem. The specimen was subjected to plain radiographic study. Histo- pathological examination also was carried out on a piece of the ossified tissue.
Observations
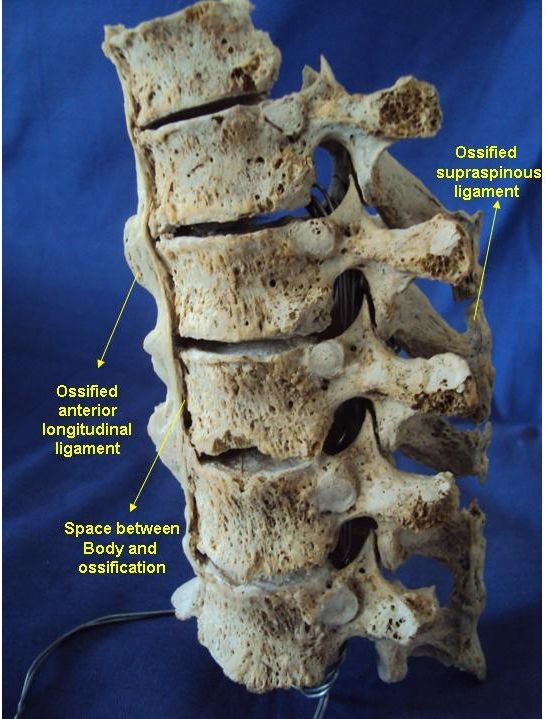
Gross examination revealed a tortuous mass anteriorly along the sides (prominent on the right side) of the vertebral bodies holding them together. A clear space was noted between the mass and the vertebral bodies. The spinous processes were also found to be held together by a similar tortuous mass (Fig. 1). The gross appearance of the mass was like that of candle wax dripping down the spines. The intervertebral disc space was found to be maintained and the zygoapophyseal joints were found to be free (Fig. 2). The intervertebral foraminae and vertebral canal appeared normal. Other parts of the vertebrae including the pedicles, laminae, transverse processes and the costal facets also appeared normal. The anteroposterior and lateral views of radiographs showed the mass to be of bony nature. It was found to be separated from the body of the vertebrae indicated by a space and radiodense line paralleling the longitudinal axis of the vertebrae (Fig. 3). The inter-vertebral disc space and zygapophyseal joint space were free. Histo-pathological examination confirmed the tissue as ossified (Fig. 4).
Fig.1 Shows six thoracic vertebrae held together by ossified anterior longitudinal ligament
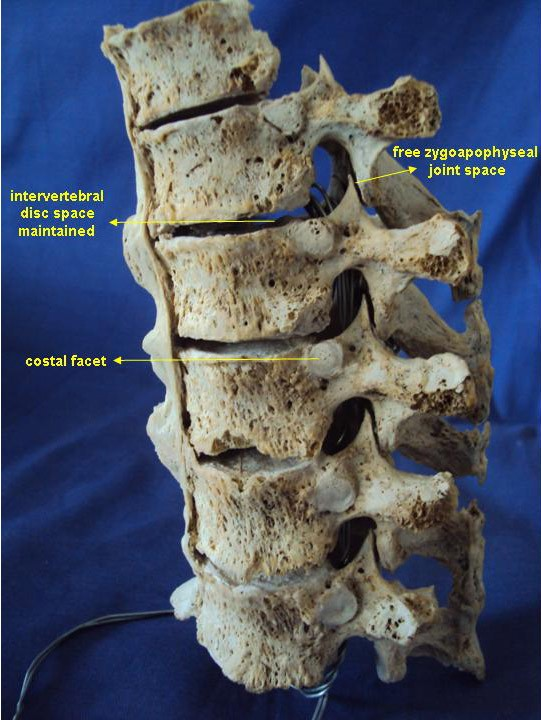
Fig. 2 Intervertebral disc space and zygoapophyseal joint space are maintained. and supraspinous ligament
Discussion
The differential diagnosis of paraspinal ligament ossification includes Forestier’s disease, Ankylosing spondylitis and Rheumatoid spondylitis (Khozaim Nakhoda and Grays, 2009). Other associated problems like fluorosis, ossified posterior longitudinal ligament (OPLL), hypophosphatemia and hypoparathyroidism need to be considered. The present observation of ossification along the anterolateral aspect of the vertebral body involving more than four thoracic vertebrae,
Fig. 3 Anteroposterior and lateral views showing bone pattern (H&E, 10X)
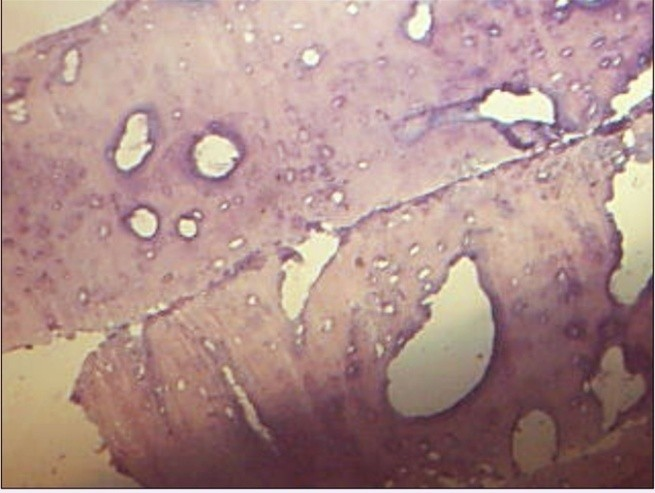
Fig. 4. Histology of mass showing lamellar ossified ligaments and radiodense line

supraspinous ligament ossification, main- tained disc space, free facetal joints, separation of the ossified mass from the body and candle wax dripping appearance favour the diagnosis of Forestier’s disease otherwise known diffuse idiopathic skeletal hyperostosis (DISH).
DISH is an idiopathic rheumato- logical abnormality in which exuberant ossification occurs along the ligaments (McCafferty et al., 1996). The incidence of this disease is about 6 – 12 % (Khozaim Nakhoda and Grays, 2009) and shows a male predominance (Westerveld et al.,2008). It is noted predominantly in elderly individuals usually after 50 years. But some had observed paediatric cases with ossification of anterior longitudinal ligament of cervical spine (Coakley et al., 1995). Although DISH commonly affects the anterior longitudinal ligament, ossification of posterior longitudinal ligament of the cervical spine is also noted in 2% of Japanese and 0.16% of Whites by Ono et al., (1982). However the pathophysiology of this phenomenon remains unknown.
DISH is found in 1-3 % of baboons, monkeys, gorillas, bears, camels, horses (Bjorkergren et al., 1985; Ferigolo, 1988; Rothschild and Woods, 1988). It is interesting to note that paleontologic records showed DISH in dinosaurs and early mammals (Rothschild, 1987; Rothschild and Berman, 1991). DISH is usually asymptomatic. Reduction in range of spinal movement may occur if vertebral fusion is extensive (Olivieri et al., 2007).
References
Bjorkergren AG, Sartoris DJ, Shermis S (1987) Patterns of aravertebral ossification in the prehistric saber toothed cat. Am J Roentgenol,148: 779-782.
Coakley FV, Vive J, Finlay DB, Shannon RS (1995) Childhood ossification of the anterior longi- tudinal ligament of the cervical spine. Clin Radiol, 50: 115 – 116.
Ferigolo J, Estudos (1988) Multidisciplinares. In: Goncalves de Araujo AJ, Ferreira LF, eds. Non human Vertebrate Paleopathology. Brazil: Panorama. 213 – 234.
Heylings DJA (1978) Supraspinous and interspinous ligaments of the human lumbar spine. J Anat,125: 127 – 131.
Khozaim N, Grays (2009) Diffuse Idiopathic Skeletal
Hyperostosis, e- Medicine Radiology / article /388973 – overview.
McCafferty RR, Harrison MJ, Tamas LB, Larkins MV (1991) Ossification of the anterior longitudinal ligament and Forestier’s disease: an analysis of seven cases. J Neurosurg, 85: 524 –525.
Olivieri , Dvingelo S, Cutro MS, Padula A, Peruz G, Montaruli M (2007) Diffuse idiopathic skeletal hyperostosis may give the typical postural abnormalities of advanced ankylosing spondylitis. Rheumatology, 46: 1709 – 1711.
Ravichandran et al., Diffuse idiopathic skeletal hyperostosis Ono M, Rusell WJ, Kudo S (1982) Ossification of the thoracic posterior longitudinal ligament in a fixed population. Radiological and neurological manifestations. Radiology, 143: 469-474.
Rothschild BM (1987) Diffuse idiopathic skeletal hyperostosis as reflected in the paleontologic record: dinosaurs and early mammals. Semin Arthritis Rheum, 17: 119-125.
Rothschild BM, Woods R (1988) Old World spondylarthropathy: the gorilla connection. Arthritis Rheum, 31: 934 – 935.
Rothschild BM, Berman D (1991) Fusion of caudal vertebrae in late Jurassic Suropods. J Vert Paleonlol, 11: 29 – 36.
Westerveld LA, Van-Ufford HM,Verlaan JJ, Oner FC (2008) The prevalence of diffuse idiopathic skeletal hyperostosis in an outpatient population in the Netherlands. J Rheumatol, 35: 1635-1638.
Williams PL, Bannister LH, Berry MM, Collin P, Dyson M, Dussek JE, Ferguson MWJ (1995) Gray’s Anatomy, 38th Edition, New York: Churchill Livingstone. 512-514.