International Journal of Anatomical Sciences 2012, 3(1):14-16
Case Report
A Rare Anatomical Variation in Medial Root of Azygos Vein with its
Embryological Aspect
Seema, Anupama Mahajan
Department of Anatomy, Sri Guru Ram Das Institute of Medical Sciences & Research, Mehta Road, Valla, Amritsar 143 501, Punjab, India
Key Words: azygos, mediastinum, hemiazygos, embryological.
Abstract: The azygos system of veins arises from the vessels in the abdomen and passes into the thorax to form paired trunks that serve as the chief drainage for the abdominal wall and for the contents of the posterior mediastinum. Because of the complex embryological development of these veins many possible variations may be expected to occur. During routine dissection for the azygos system of veins the present adult male cadaver of unknown age was found to have an anatomical rare variation in the formation of the azygos vein. The medial root of formation of azygos vein showed Y shaped pattern and contributed to both azygos and hemiazygos vein formation. The embryological basis of this variation was studied and discussed. The rest of the azygos venous system did not show any variation. These embryological variations are important for the mediastinal surgeons and radiologists to avoid misinterpretations.
A number of variations of the azygos venous system are reported (Celik et al.,1996) which are due to its complex embryological development (Mezzogiorno and Passiate, 1988). The azygos vein has its origin in the thorax at the level of twelfth thoracic vertebra by the union of three roots Lateral root, Intermediate root and Medial root.
Lateral root is the common trunk formed by the union of right ascending lumbar vein and right subcostal vein in the thorax just below the head of twelfth rib (O’Neil, 1945). The right ascending lumbar trunk begins in the pelvis, connects with the lumbar veins, inferior vena cava and right
Intermediate root also known as lumbar azygos is a vein which usually arises from dorsal aspect of the inferior vena cava. It passes upwards and joins the lower end of azygos vein (Seib, 1934). Medial Root is the communicating vein which communicates caudally with the inferior vena cava or left renal vein and with the intermediate azygos root cranially. Sometimes it arises from the dorsal aspect of the inferior vena cava as common medial root which passes through the aortic opening of diaphragm into the thorax and immediately divides into two branches known as medial azygos and medial hemiazygos root of origin which terminates in the caudal extremity of the azygos and hemiazygos venous forming a Y shaped pattern (Seib, 1934). It is important to keep in mind that different courses of the azygos system do exist so that extra caution is required during surgery of the mediastinum and also in appropriately interpreting the radiographs (Brenner et al., 1974).
Case Report
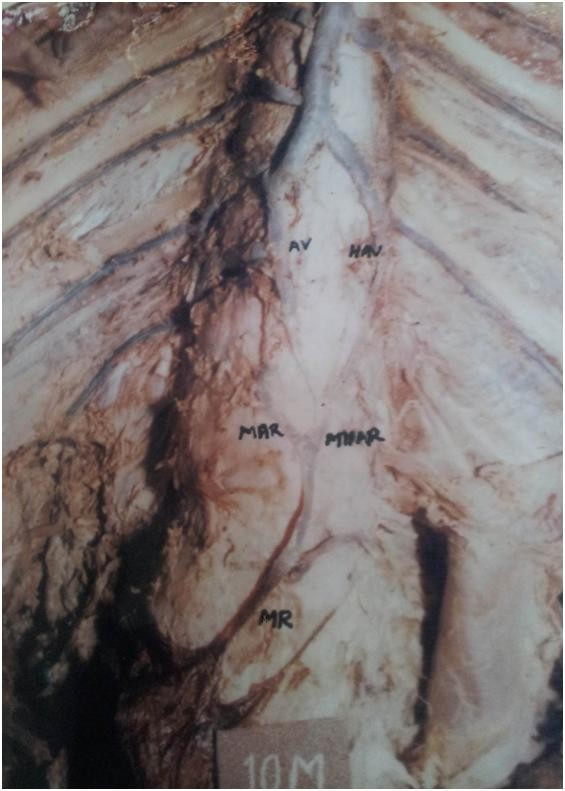
During routine dissection of the posterior thoracic wall for the azygos system of veins in an adult human cadaver we encounter a variation in the formation of the azygos vein. The medial root of the formation of the azygos vein arose from the inferior vena cava, ran upward closely applied to the vertebral column. Opposite the twelfth thoracic vertebra it divided into two branches namely medial azygos and medial hemiazygos root. These joined the caudal ends of the azygos and hemiazygos vein respectively. The hemiazygos immediately drained into azygos vein. All the other major vessels like superior and inferior vena cava were normal.
|
Photograph showing Medial root (MR) arising from the inferior vena cava and dividing into medial azygos (MAR) and medial hemiazygos (MHAR) joining the azygos vein (AV) and hemiazygos vein (HAV) respectively
Discussion
The azygos venous system has very complex embryological origin so many possible variations may be expected to occur (Ozbek et al., 1999). Medial azygos root arises from the dorso medial aspect of the inferior vena cava at or below the left renal vein usually opposite the second lumbar disc and entered the thoracic cavity through the aortic opening of the diaphragm dividing immediately into two branches which were named as Medial azygos root present on the right side formed the azygos vein by joining the lateral root. Medial hemiazygos root present on the left side formed the hemiazygos vein by joining the left lateral root. To understand the embryonic derivation of the Y thus formed by the bifurcation of the common medial root let us suppose that the twelfth retro aortic anastomosis, persisted in its entirety and also that the right sub central vein remained from this level caudally forming a T-shaped pattern. But since the establishment of the definitive arrangement probably takes place early in intrauterine development, it is possible that as a result of various growth and hydro dynamic factors, the twelfth retro aortic anastomosis may be pulled slightly caudally at the point where the sub-central vein meet it, forming a Y shaped pattern with a very shallow fork and with almost horizontal arms. Thus it would seem that the arms of the Y in these shallow and most simple patterns are formed chiefly from a retro-aortic anastomosis. To explain the patterns having a deep and long armed fork, let us assume that the following venous segments persist
1. The right and left medial sympathetico- subcentral anastomosis at the level of the 12th thoracic intersegmental veins, The
(right medial sympathetic line-right subcentral line) and Th12 (left medial sympathetic chain-left subcentral vein)
2. The right and left subcentral veins between the levels of the 12th thoracic and second lumbar intersegmental veins, right sub central line (Th12-L2) and left subcentral vein (Th12-L2)
3. The inter sub central anastomosis at the level of the second lumbar intersegmental vein, L2 (right subcentral line-left subcentral line).
4. The right subcentral between the levels of the second and third lumbar intersegmental veins, right subcentral line (L2-L3).
The right medial sympathetico-sub central anastomosis at the level of the third lumbar intersegmental veins (L3 right medial sympathetic line-right subcentral line). The right medial sympathetic para ureteric anastomosis at the same level L3 (right medial sympathetic line-right thoracolumbar line).
The results will be a Y-shaped pattern with a deep long armed fork, or in adult terminology, a common medial root of origin arising from the inferior vena cava at the level of L3 and passing cranially to bifurcate quickly at the level of L2.Each of the branches then continues obliquely cranially and laterally, the right to terminates in the beginning of the azygos vein (medial azygos root), left in the hemiazygos (medial hemiazygos root). The right branch in this example is formed almost entirely from the right subcentral vein; only a short horizontal segment occurring at its cranial extremity. The left branch was chiefly formed from the left subcentral but with short horizontal segments at either extremity. The cranial portions of the lumbar medial sympathetic veins could constitute the cranial portion of these branches just as well as the subcentral veins of this example (Seib, 1934). Surgeons should be aware of these variations during mediastinal operations of the possibility of variations of the azygos venous system to avoid profuse bleeding. Also the congenital venous malformations may be one of the causes of thromboembolic disease especially in young people with no other associated risk factors for thromboembolism (Ordonez et al., 1999). The variant azygos veins which are continuous with the inferior vena cava are associated with anomalies of heart, spleen and superior vena cava (Minniti et al., 2002). These can also cause confusion in diagnosing these structures after detection in scans and MRI (Smathers et al., 1983).
Conclusion
The knowledge of the anatomical variations of the azygos vein is very helpful to the mediastinal surgeons to identify the variable structures so that inadvertent hemorrhagic complications can be avoided. Also they will avoid confusion in diagnosing the structures on radiographs and MRI scans
References
Brenner BJ, Darling RC, Frederick PL, Linton RR (1974) Major venous anomalies complicating abdominal aortic surgery. Arch Surg, 108: 159-165.
Celik HH, Sargon MF, Aldur MM, Cumhur M (1996) An anomalous course of the interazygos vein. Surg Radiol Anat, 18: 61-62.
Mezzogiorno A, Passiate C (1998) An atypic pattern of the azygos venous system in man. Anat Anz,165: 277-281.
Minniti S, Visentini S, Procacci C (2002) Congenital anomalies of the venae cavae: embryological origin, imaging features and report of three new variants. Eur Radiol, 12: 2040-2055.
O’ Neil EE (1945) Ligation of the inferior vena cava in the prevention and treatment of pulmonary embolism. N Engl J Med, 232: 641-646.
Ordonez FS, Carrasco JCG, Recio FJB, Cuevas RA, Lopez TF, Santos PG (1998) Absence of the inferior vena cava causing repeated deep venous thrombosis in an adult: a case report. Angiology,49: 951-956.
Ozbek A, Dalçik C, Colak T, Dalçik H (1999) Multiple variations of the azygos venous system. Surg Radiol Anat, 21: 83-85.
Seib GA (1934) The azygos system of veins in American Whites and American Negroes including observations on the inferior caval venous system. Amer J Phys Anthrop, 19: 39-163.
Smathers RL, Lee JK, Heiken JP (1983) Anomalous preaortic interazygos vein. J Comp Assist Tomogr, 7: 732-733.
Standring S (2008) In Gray’s Anatomy. 40th Edition,Churchill Livingstone, London; pp939-940.