International Journal of Anatomical Sciences 2012, 3(1): 19-21
Research Article
Martin-Gruber Anastomosis – Its Morphology and Clinical significance
Azhagiri R, Melani Rajendran S.
Department of Anatomy, Sri Muthukumaran Medical College Hospital and Research Institute, Chikkarayapuram, Chennai 600 069, Tamil Nadu, India.
Department of Anatomy, Sri Ramachandra Medical College and Research Institute, Porur, Chennai 600 116, Tamil Nadu, India.
Key words: Martin-Gruber, anastomosis, ulnar nerve, median nerve
Abstract: Knowledge on the prevalence of variations between the nerves is essential when establishing the diagnosis of neuropathies and surgical landmarks. In this study,50 forearm regions of cadavers of both sexes were dissected to examine the communication between the median and ulnar nerves (Martin-Gruber anastomosis). This anastomosis was found only in one case (2%) on the left side. There was no significant gender in the incidence of this connection. Despite the low incidence of Martin-Gruber anastomosis been observed here, the importance of an adequate investigation of these connections needs to be understood.
Martin- Gruber anastomoses are the communications of motor nerve fibres in the forearm between the median and ulnar nerves. Most of the communications cross from the median nerve to the ulnar nerve (Rodriguez-Niedenfuhr et al., 2002) and are bilateral in 10 to 40% of the cases (Taams,1997). Martin- Gruber anastomoses was first demonstrated by the anatomist Martin in 1763, and later by Gruber in 1970 (Gruber,1970). When present, it is unilateral and occurs more frequently in the right arm. Martin-Gruber Anastomosis apparently carry only motor fibres (Leibovie et al.,1992, Hasegawa et al.,2001).
This anomaly is asymptomatic and often goes undetected. However, its presence is detected with injuries or other disturbance of ulnar or median nerve (Iyer,1976). Understanding the existence of this variation, its location and its possible presentation is important for correct patient assistance. Therefore the study was carried out to find out the prevalence of such anastomosis.
Material and Methods
Upper limbs from 20 cadavers of both sexes (40 nos) and 10 free upper limbs were used for the study. The dissection has been done on both sides of the upper limbs to expose the flexor surface of forearm. The flexor muscles were exposed and the ulnar and median nerves and their branches were exposed and the anatomical arrangement and the relationship with adjacent structures were observed to find out the presence of Martin- Gruber anastomoses.
Observations
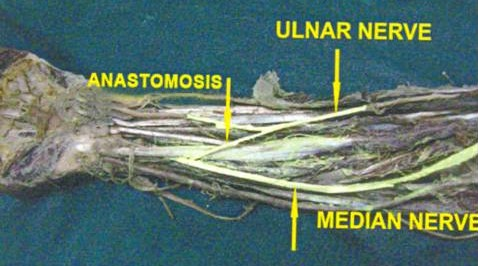
Out of 50 cases dissected, only one case (2%) showed the presence of Martin – Gruber anastomosis on the right side in the distal part of proximal half of the forearm. The communicating fibers were traversing from the ulnar to the median nerve (Fig.1).
Fig. 1 Martin-Gruber anastomosis in the lower one third of the left forearm
Discussion
The Martin – Gruber anastomosis (Gruber, 1870) is a communication between the motor fibers of the median nerve or its branches and the ulnar nerve in the forearm which occurs in 15% of limbs.In the present study, 2% of the cases the Martin – Gruber anastomosis it was found between median nerve and ulnar nerve in the proximal part of distal third of forearm.Such anastomosis occurs in 15% of the limb, it is being derived from the AIN in 50% of cases (Collins and Weber, 1983). Mannerfelt (1966), observed approximately one Martin–Gruber anastomosis in two cases arose from the AIN, therefore a lesion of that nerve can sometimes cause weakness of the ulnar innervated small muscles of the hand.
In Hirasawa’s study (1931), this type of communication was found in 10.5% of forearms. Maeda et al., (1977) stated that one half of these communications arise from the AIN. Incidence of this communication was 5% in his study of Frazao et al (2000), the present study also coincides with this. Kaplan (1984) described the Martin–Gruber anastomosis as a motor anastomosis spreading from the median to the ulnar nerve in the forearm, whereas Ranschburg and Ober die (1917) described it as a transfer of motor as well as sensory fibers from the median to the ulnar nerve. On the contrary, in the present observation there was transfer of fibers from the ulnar to the median nerve. Such transfer of fibers from the ulnar to median nerve is extremely rare (Amoiridis,1992). Martin–Gruber anastomosis has clinical importance. The major danger in not recognizing Martin–Gruber anastomosis is that of mistakenly interpreting the findings as ulnar conduction block. Apart from it Martin–Gruber anastomosis has clinical significance for understanding median nerve lesion and carpel tunnel syndrome. It appears from the present study that identification of Martin–Gruber anastomosis is very crucial before labeling the condition as ulnar neuropathy as the mode of treatment differs accordingly (former needs no treatment while later need it appropriately). Further, we concluded that nerve conduction study is a reliable tool diagnosis of Martin– Gruber anastomosis prevalence of which we reported as 12% in central Indian subjects.
References
Amoiridis G (1992) Frequency of ulnar-to-median nerve anastomosis. Electromyogram. Clin Neurophysiol, 32: 255-256.
Collins DN, Weber ER (1983) Anterior interosseous nerve syndrome. South Med J, 76: 1533–1537.
Frazao R, Alves N, Cricenti SV (2000) The origin and point of penetration of the nerve branches supplying the flexor digitorum profundus. Braz J Morphol, 17: 113-116.
Gruber W (1970) Uber die Verbindung des Nervus medianus mit dem Nervus ulnaris am Unterarm des Menschen und der Sfiugetiere. Arch Anat Physiol, 37: 501-522.
Hasegawa O, Matsumoto S, Iino M, Kirigaya N, Mimura E, Wada N, Gondo G (2001) Prevalence of Martin-Gruber anastomosis on motor nerve conduction studies. No To Shinkei, 53: 161-164.
Hirasawa K (1931) Untersuchungen iiber das periphere Nervensystem, Plexus brachialis und die Nerven der oberen Extremititen. Arb Anat Inst Kaiseflichen Univ Kyoto, A2: 135-137.
Iyer V, Fenichel GM (1976) Normal median nerve proximal latency in carpal tunnel syndrome: a clue to coexisting Martin-Gruber anastomosis. J Neurol Neurosurg Psychiat, 39: 449-452.
Kaplan EB (1984) Nerve supply to the muscles and skin of the hand. In: Kaplan’s functional and surgical anatomy of the hand, 3rd ed. Lippincott, Philadelphia, pp 238-24l.
Leibovic SJ, Hastings H (1992) Martin-Gruber revisited. J Hand Surg, 17: 47-53.
Maeda K, Miura T, Komada T, Chiba A (1977) Anterior interosseous nerve paralysis report of 13 cases and review of Japanese literatures. Hands,9: 165–171.
Mannerfelt L (1966) Studies on the hand in ulnar nerve paralysis. A clinical experimental investigation in normal and anomalous innervation. Acta Orthopaedics Scandinavica, suppl. 87: 23-25 and 130-142.
Ranschburg P, Ober die (1917) Anastomosen der oberen Extremitit des Menschenmit Rticksicht auf ihre neurotogische und nervenchirurgische Bedeutung. Neurol Zentralbl, 13: 521.
Rodriguez-Niedenführ M, Vazquez T, Parkin I, Logan B, Sañudo JR (2002) Martín-Gruber anastomosis revisited. Clin Anat, 15: 129-134.
Taams KO (1997) Martin-Gruber connections in South Africa. An anatomical study. J Hand Surg,22B: 328–330.