International Journal of Anatomical Sciences 2012, 3(1): 04-07
Case Report
A Case of Unilateral Renal Agenesis in a Female
Arun Kumar S. Bilodi, Gangadhar M.R.
Department of Anatomy, Mahatma Gandhi Medical College and Research Institute, Pillaiyarkuppam, Pondicherry 607 402, India.
Department of Anthropology, University of Mysore, Manasagangothri, Mysore 570 006, Karnataka, India.
Key Words: agenesis of kidney, renal fossa, absence of kidney, ectopic kidney, single kidney, inherited renal anomaly, ureteric bud
Abstract: Agenesis of kidney is the absence of either left or right kidney .If absent on both sides it is incompatible with life. Absence of kidney on one side will not produce any symptoms because other kidney may be enlarged and renal functions will not be affected. This anomaly was detected during routine investigation for pain in abdomen. This is a case of unilateral absence of kidney on the side in a female aged about 45 years diagnosed during routine investigation by ultrasound of the abdomen at Raja Rajeswari Medical College and Teaching Hospital at Bangalore for pain in abdomen, vomiting and tenderness in the right Hypochondrium. Ultrasound did not reveal any other anomaly. All the other abdomino-pelvic organs were normal in the mother of two children with no systemic diseases. Since it is a case of solitary agenesis of one kidney with no other associated anomalies, it has been studied and reported.
Renal agenesis may occur when there is failure of interaction of metanephric mesoderm and ureteric bud. GDNF is produced normally during interaction by metanephric mesoderm that produces branching and growth of ureteric bud. When mutation occurs, in genes that controls signaling of GDNF expression, this will give rise to agenesis of kidney. There may be common associated congenital defects like cardiac anomalies, atresia of trachea and duodenum, cleft lip and cleft palate and anomalies of brain. In Potters disease there is characteristic appearance of flattened face of the fetus, beak like nose and anomalies of foot. Incidence of bilateral agenesis is 1 in 10,000 live births resulting in renal failure (Saddler, 2009). Agenesis of kidney is observed in 20% of same side and 0.5 % of cases on contra lateral side (Dursun et al.,2005)
Case report
A 45 years old female visited the surgical outpatient department with a history of abdominal pain for one week in the right hypochondriac region at Raja Rajeswari Medical College and Teaching Hospital, Bangalore in the month of November 2009. No history of vomiting fever and other complaints were registered. Clinical examination did not reveal any palpable mass both in pelvic region and nor in lumbar region and right hypochondriac region. Other systems examined were within normal limits
Family history
There was positive family history of renal congenital anomalies. Her elder brother had Horse shoe shaped kidney – where both the kidneys were fused in their lower poles. This anomaly was also detected during his routine investigations for his diabetes .He was not hypertensive. Later he died of Cirrhosis of liver and portal hypertension. Other members of her family did not have any renal anomalies.
Personal history
Mother of two male children both delivered by Caesarean section due to Transverse Lie in the first pregnancy and Ante Partum Hemorrhage (APH) in her second pregnancy. She was neither diabetic nor hypertensive.
Investigation
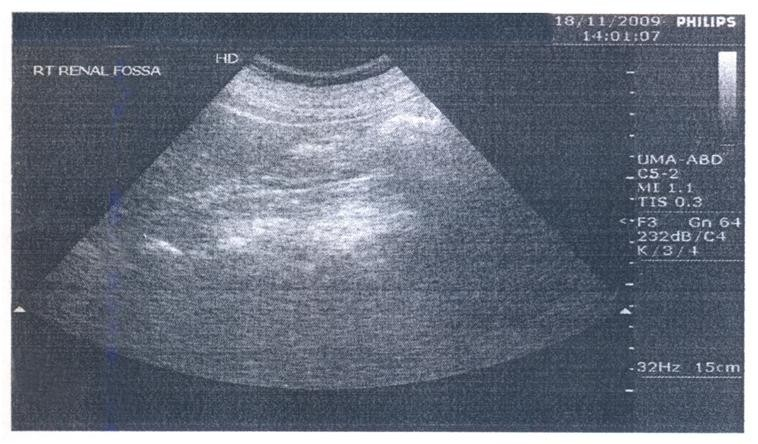
Later routine blood examination and urine examination along with ultrasound of the abdomen were done. Blood examination revealed anemia (Hemoglobin 8 gm%) and hence she was feeling fatigue. Other values were normal. Urine examination revealed neither infection nor sugar in the urine. Ultrasound of the abdomen revealed non visualization of right kidney in the renal fossa or in the pelvis; while left kidney measured 9.9 cm with parenchymal thickness of 1.7 cm, normal in size, shape and echo texture. Cortico-medullary differentiation was well maintained. There was no evidence of caliculi or calyceal dilatation. All other organs were normal. She was advised to undergo intra venous pyelogram; however was not carried out as she was sensitive to dye or contrast.
Impression
Absence of right kidney.
DISCUSSION:-
Congenital anomalies of urinary tract including kidneys form the important causes of renal insufficiency during childhood (Flvush et al., 1998). Renal agenesis may be either unilateral or bilateral renal agenesis or dysgenesis is not only rare but incompatible with life with an incidence of 1 or 2 per 10,000 live births in the male to female ratio of 3:1. About 20-36% have familial tendency (Mishra, 2007). Congenital absences of kidney in patients were primarily due to agenesis and partly because of renal aplasia (Woolf and Winnyyard,1998; Doroshow and Abeshouse, 1961). Even autopsy studies have shown congenital absence of kidneys predominantly due to renal agenesis (Fortune, 1927).
Fig. 1 Ultra-sound photograph of the abdomen showing non-visualization of right kidney. (Absence of kidney in the right renal fossa)
Mishra, (2007) reported a case of unilateral renal agenesis in a male aged 30 years with history of pain abdomen of 6 months duration in the outpatient department of surgery who was hale and healthy. On routine ultrasound examination revealed an empty renal fossa on the right side and left kidney showed compensatory hypertrophy. There was associated presence of ipsilateral genitourinary anomalies like dilated ureter seminal vesicle hypoplasia. Vas deferens was also absent. In Vater syndrome, there were developmental abnormalities of vertebrae, ventricular septal anomalies, atresia of anorectal region, lesions of trachea and esophagus and radial bone abnormality (Mishra, 2007).
Ghifr et al., (2007) reported a case of non visualization of left kidney in a 16 years old girl with a history of pain in the right lumbar region. She was febrile, on clinical examination her abdomen was soft with no palpable mass associated with free lumbar pits, and normal external genitalia. X-ray abdomen did not show any significant findings. Ultrasonography showed dilatation of pelvis and major calyces of right kidney, and non visualization of left kidney. Her renal function test was normal with sterile urine. Intra venous pyelogram (IVP) showed absence of secretion and excretion in the left side until 16th hour after injection of contrast product with right junction syndrome. Te99mDMSA renal sciantigraphy showed absence of uptake of tracer compared to the left renal confirming the diagnosis of right renal agenesis (Ghifr et al., 2007) Masahiro Hiraoka.et al., (2002) diagnosed multicystic dysplastic kidney in one patient, renal aplasia in three patients and renal hypoplasia in five patients by ultrasound measurements. Potter (1965) stated that unilateral agenesis unlike renal aplasia was often complicated by anomalies of internal genital organs especially in females and occasionally in other organs other than genito urinary anomalies (Potter, 1965). Incidence of congenital solitary kidneys by ultra sound screening on the random newborns showed an incidence of one in 1300 new born. But there was no renal agenesis. Potter observed that unlike renal aplasia, unilateral agenesis of kidney was complicated by abnormalities of internal organs also (Potter, 1965). Ipsilateral agenesis of adrenals was seen in 8-10% cases (Mishra, 2007). When ureteric bud fails to develop, then agenesis of kidney is produced. Metanephric tissues will not be differentiated into nephron in the absence of urteric bud. Occasionally there is dilated ureter seminal vesicle hypoplasia and absence of vas deferens as seen in Vater syndrome. There were no developmental abnormalities like vertebral, ventricular septal anomalies, atresia of anorectal region, lesions of trachea and esophagus and radial bone deformity as seen in Vater syndrome. Unlike renal aplasia, there was no ipsilateral agenesis of adrenals or multicystic dysplastic kidney. There are no systemic diseases. Since it is a pure solitary case of agenesis of right kidney and normal left kidney with positive family history of renal anomalies (horse shaped kidneys), it has been reported for its rarity.
Acknowledgements
The Author wishes to thank the Medical Director, and HOD Surgery of Raja Rajeswari Medical College, Bangalore.
References
Doroshow L, Abeshouse B (1961) Congenital unilateral solitary kidney. Report of 37 cases and review of literatures. Uro Surv, 11:219-226.
Fivush B, Jabs K, Neu AM, Sullivan EK, Feld L, Kohaut E, Fine R (1998) Chronic renal insufficiency in children and adolescents. The 1996 annual reports of NAPRTCS. Pediatric Nephrol, 12: 328-337.
Fortune C (1927) The pathological and clinical significance of congenital one sided kidney defect with 3 new cases of agenesis. Ann Internal Medicine, 1:377-399.
Ghifr I, Fellah S, Rais NB (2007) Unilateral renal agenesis revealed by hydro nephrosis of contralateral kidney and explored by 99mTc-99m
Dursun H, Bayazit B, Buyukeelik M, Soran M, Noyan A, Anarat A (2005) Associated anomalies in children with congenital solitary functioning kidney. Pediatr Surg, 21: 456-459.
Masahiro H, Tsukahara HY, Ohshima Y, Kasuga K, Ishihara Y, Mayumi M (2002) Clinical nephrology, epidemiology, clinical trials. Kidney Internationals, 61: 1840-1844.
Mishra A (2007) Renal agenesis–Report of an interesting case. British J Radiol, 80: e167-e169.
Potter E (1965) Bilateral absence of ureters and kidneys. Obst Gynecol, 25: 3-12
Sudhir SS (2008) Embryology for medical students- Urogenital systems. 2nd Edition. Jaypee brothers, New Delhi.pp 239.
Woolf A, Winnyyard P (1998) Adavances in the cell biology and genetics of human kidney malformations. J Am Soc Nephrol, 9: 1114-1125.