International Journal of Anatomical Sciences 2011, 2(2):19-21
Case Report
Crossed Fused Renal Ectopia – a Case Report
Rajaram V, Govindarajan M.
Institute of Anatomy, Madurai Medical College, Madurai 625 020, Tamilnadu, India.
Key words: crossed renal ectopia, nephrolithiasis, accessory renal artery
Abstract: Ectopic kidney occurs as a result of a halt in migration of kidneys to their normal location, during the embryonic period. Due to their ectopic position and aberrant vascularity, they are more prone to many diseases such as urinary tract infection, renal stones, hypertension etc. The clinical features are not peculiar of renal diseases and needs sophisticated investigations to fix the exact diagnosis. A case report about an ectopic fused kidney is presented here for its rarity and clinical significance.
In adult, the kidneys are situated in the lumbar region as a retroperitoneal organ. They originate in pelvic cavity from the metanephros during the embryonic period. Due to rapid differential growth of the caudal end of the embryo, they migrate cranially and rotated medially to reach their final location.
Crossed fused renal ectopia refers to a rare congenital anomaly (Daniel and Datnow,1977; Debnath et al., 2003; Boyan et al.,2007); where the kidneys are fused and located on the opposite side of the midline in relation to its ureteric orifice in the urinary bladder. The estimated incidence of this anomaly is around 1 in 1000 live births, with male predilection of 2:1. In addition to that, left to right ectopy is three times more common.
Renal ectopic may present a diagnostic problem when it get diseased acutely, because the clinical features are different from that of produced by the normally located kidney. A case of ectopic fused kidney is presented here for its rarity and clinical significance.
Case Report
During routine cadaver dissection, in the dissection hall of the Institute of Anatomy, Madurai Medical College, we came across a mass in the right iliac fossa of 50 year old male cadaver. While analyzing the mass we confirmed that it was a fused renal mass. Understanding the rarity of the specimen we carefully dissected and recorded its position, relations and blood supply. Photographs were taken for documentation (Fig. 1).
The fused ectopic renal mass in the right iliac fossa showed following anatomical features: the renal mass was situated in front of the right iliacus muscle and sacrum and partly in the right pelvic brim. Careful analyzes revealed that the left kidney crossed the midline and came to occupy the right iliac fossa and right kidney failed to ascend and present in the same right iliac fossa. Both the kidneys were fused transversely and appeared like a disc in shape. Two distinct hila were seen; one at 1cm right-lateral to the midline and other was present in the right end of the renal mass. There were two renal arteries from the aorta just before its bifurcation infront of 20IJAS 2011, 2(2): 19-21 the sacral promontory, and entered the respective hilum. In addition there was a small accessory renal artery from the left common iliac artery which entered the left end of the renal mass. Corresponding renal veins drained in the inferior vena cava and left common iliac vein. Right ureter had normal anatomical course, but the left ureter crossed the midline and passed behind the sigmoid colon and both ureters opened typically in the urinary bladder. Supra renal glands were present in the normal anatomical position with reference to kidneys and there was no change in their vascularity. No other anomalies were noted.
Fig. 1 Ectopic Fused Kidney

Fig. 2 Renal arteries to the fused ectopic kidney
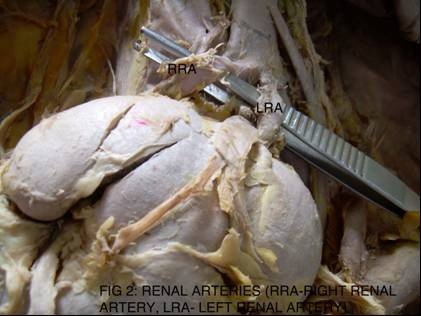
(RRA – Right Renal Artery; LRA – Left Renal Artery)
DiscussionRenal fusion and anomalies were first studied and classified by Wilmer, (1938) later it was revised by McDonald and McClellan,(1957). They classified the ectopic sequel into four major types as
1. Crossed ectopia with fusion
2. Crossed ectopia without fusion.
3. Solitary crossed ectopia and
4. Bilaterally crossed ectopia.
Crossed ectopia with fusion type is further sub classified into
1. Unilateral fused kidney with inferior ectopia : in which the crossed kidney lies inferior to the resident kidney. The upper pole of the crossed kidney is fused to the lower pole of the resident kidney
2. Sigmoid (or) S shaped, kidney: The crossed kidney lies inferiorly with its pelvis directed laterally. The pelvis of the superiorly located resident kidney is directed medially.
3. Unilateral lump kidney: The kidneys are fused along their medial borders. The renal pelvis of the resident kidney is directed anteromedially and the crossing renal pelvis directed laterally.
4. L shaped kidney: The crossed kidney lies inferiorly and transversely.
5. Unilateral fused kidney with inferior ectopia. The crossing kidney lies superior to the resident kidney. Both renal pelvises are anteriorly rotated.
In our specimen the fused mass was disc shaped both pelvises were directed antero medially.
The factors responsible for this type of ectopia and fusion were still undetermined. However, Wilmer (Year) suggested that Rajaram and Govindarajan – Crossed Fused Renal Ectopia 21 IJAS 2011, 2(2): 19-21 crossover occur as a result of pressure from abnormally positioned umbilical arteries that prevent the normal ascent of the kidney which then follows a path of least resistance to the opposite side.
Some more proposed theories are:
A. Faulty ureteric bud development. B. Teratogenic factors.
C. Abnormal variation in the growth of the hind gut.
D. Abnormal position of the caecum.
However mechanical factors alone do not provide comprehensive explanation. When one considers that cardio vascular and skeletal anomalies associated with renal ectopia. Most of the time, the renal ectopia is associated with Vertebral, anorectal, cardiac, trachea – oesophagel, renal and limb (VACTERL) anomalies (Gray and Skandalakis 1972; Russell et al., 2000).
More than one anomaly can occur at the same time, while kidney ascend through the pelvis they receive new arterial branches from vessels (iliac / aorta) close to them. When they finally reach the lumbar region they receive the new branches from abdominal aorta and the former branches degenerate . In ectopic kidney they don’t degenerate and present as accessory renal arteries. Several studies showed that hypertension is more frequently encountered in cases with more than one renal artery in each side. These accessory renal arteries may compress the pelvis and ureter and can produce obstructive hydronephrosis. In our study there was one accessory renal artery from left common iliac artery which entered the left and of the renal mass which may be the non-degenerated portion of the embryonic accessory renal artery. Thus gives an indication that the prelude to the anomalous pattern of kidneys seen in this study could embryologically originated from this accessory renal artery.
Conclusion Most patients with renal ectopia do not have symptoms and are diagnosed incidentally. But these anomalies are more prone to develop recurrent urinary tract infections (due to stasis), nephrolithiasis, trauma, hydroneph- rosis and hypertension (due to anomalous vasculature). The ectopic kidney when diseased the clinical features are not classical and sophisticated investigations are needed to fix the diagnosis.
References
Boyan N, Kubat H, Uzum A (2007) Crossed renal ectopia with fusion: report of two patients. Clin Anat, 20: 699-702.
Crossed fused Ectopic Kidney – A Case Report. TAJ,16: 79-81
Daniel WW, Datnow B (1977) Crossed fused renal ectopia with renal dysplasia. Am J Roentgenol,128:845-846.
Debnath JC, Sarker KP, Uddin MN, Sarker SK, Rahman KM, Asif Rahman AM (2003)
Gray SW, Skandalakis JE. Embryology for Surgeons.
The Embryological Basis for the Treatment of Congenital Defects. Philadelphia: W.B. Saunders Co., 1972.
McDonald JH, McClellan DS (1957) Crossed renal ectopia. Am J Surg, 93: 995–1002.
Russell RCG, Williams NS, Bulstrode CJK (2000)th
Bailey & Love’s Short Practice of Surgery. 24 Edition. UK. 1174.Wilmer HA (1938) Unilateral fused kidney. A report of five cases and a review of the literature, J Urol,40: 551.
Rajaram and Govindarajan – Crossed Fused Renal Ectopia