International Journal of Anatomical Sciences 2012, 3(1): 08-11
Research Article
A Study of Dermatoglyphic Patterns in Myocardial Infarction
Rekha P, Senthil Kumar S.
Department of Anatomy, Sri Ramachandra Medical college and Research Institute, Sri Ramachandra University, Porur, Chennai-600 116, Tamil Nadu, India.
Key Words: dermatoglyphic patterns, genetic susceptibility, fingerprints & myocardial infarction.
Abstract: Coronary Artery Disease is the most important cause of morbidity and mortality in the world. The knowledge of major risk factors and its relation with genetic susceptibility serves as a screening tool in prevention of Myocardial Infarction. Fingerprint patterns of both hands were observed among 75 Myocardial Infarcted subjects and equal number of healthy subjects. This study showed that tented arch pattern in index fingers of both the hands has been well observed in Myocardial Infarcted subjects thus serving as an indicator of genetic susceptibility in the incidence of Myocardial Infarction.
Abbreviations Used: MI – Myocardial Infarction.
The types of fingerprint are unique based on the genetic characteristics of each individual. Dermatoglyphics (from ancient Greek word derma-means skin, glyph-means carving) is the scientific study of fingerprints. In humans and animals, these dermatoglyphic patterns are present on fingers, palms, soles and gives insight into a critical period of embryogenesis between four weeks and five months, when the architecture of major system is developing (Cummins et al., 1961). Generally, the pattern of fingerprint is divided into three types namely arch, loop and whorl (Fig.1). The arch type is divided to two subgroups: simple and tented and the loop type is divided to two subgroups: radial and ulnar. The whorl type is divided into five subgroups as simple, central packed loop, twinned loop, lateral packed loop, and accidental. In general population, the line pattern consists of arch type, 4% loop type 55% and whorl type 41% respectively. An extensive report has been published with regard to the relation of skin lines and various diseases for example Down’s syndrome, Schizophrenia, constipation, congenital hypodentia and bile ducts atresia. Dermatoglyphic features have been associated with numerous medical disorders (Schaumann & Alter, 1973). These associations have generated considerable interest in clinical medicine in light of their potential for providing inexpensive and noninvasive screening methods for certain disease as well as insight into the etiology of disease. The alleles that occur on different chromosomes, has been suggested by the fact that several medical and congenital chromosomal disorders produce specific alterations of fingertip patterns (Rashad et al., 1978).
Myocardial infarction (MI) commonly known as a heart attack is the interruption of blood supply to a part of the heart causing myocardial necrosis. This is most commonly due to occlusion of a coronary artery following the rupture of a vulnerable atherosclerotic plaque. This cardiovascular disease is the leading cause of mortality in the world. Early detection and screening tools are highly essential to prevent this disease thereby dermatoglyphics emerges as a clinical instrument and genetic tool of significance. High heritability, high degree of individual variations and permanence or unchanging morphology throughout post- natal life makes the dermatoglyphic pattern as an excellent prognostic and genetic marker (Rashad et al., 1975). Takashina et al., (1966) strongly suggested that an extensive analysis of palmar dermato- glyphics in patients as well as their relatives would materially aid in the study of the genetics of congenital heart disease thereby, dermatoglyphics is emerging as a clinical instrument and genetic tool of significance. This study was conducted to investigate the relation between the dermatoglyphic pattern as indicator of genetic susceptibility in patients with Myocardial Infarction.
Materials and Methods
This study was conducted in the Departments of Cardiology and Anatomy at Sri Ramachandra Medical College and Research Institute, Sri Ramachandra University, Chennai. The fingerprints of both the hands were obtained from 75 subjects with diagnosis of Myocardial Infarction who were admitted to Coronary Care Unit taken as group one and 75 healthy subjects as control, group two. The subjects were aged between 21 years to 75 years. The prior informed consent was taken from both the groups for taking the prints. The materials used for taking fingerprints were rollers, printers’ ink, and cotton, sterilium, and magnifying glass lens and proforma sheets. The data were statistically analyzed by chi square test.
Fig. 1 Types of Finger Print Patterns

Results
The loop, whorl, arch and tented arch patterns were the main patterns studied and their incidence and predominance of the pattern were observed in both the groups respectively (Fig. 2 and Fig. 3). The statisti- cally significant observations were obtained on the left index and left middle finger only in both the groups.
Fig. 2 Finger Print of Control Group
T – Thumb, I – Index, M – Middle, R – Ring, L – Little fingers
Loop: Out of total 150 subjects the loop pattern was observed higher in control group than that of Myocardial Infarction group. Radial loop Pattern was about 16% in Myocardial Infarction group and 3% in Control group and the ulnar loop was about 94% in Myocardial Infarcted group with 58% in control group.
Whorl: This pattern was significantly observed in about 60% of Myocardial Infarcted group and 58% in control group. The incidence of whorl pattern was higher in right index finger of control group and left index finger of Myocardial Infarcted group.
Arch: It was found that 21% of the Myocardial Infarcted subjects have arch pattern in thumb, index, middle and ring fingers. In contrast only 8% of the control groups have this arch pattern. Interestingly this pattern was absent in little finger of both the groups.
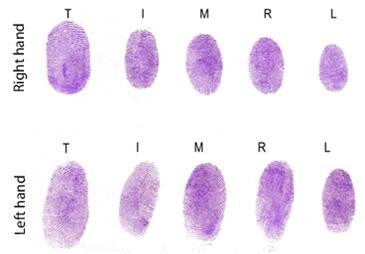
Fig. 3 Finger Print of a Myocardial Infarcted Subject


T – Thumb, I – Index, M – Middle, R – Ring & L
– Little fingers
Tented Arch: The tented arch fingerprint is significantly increased in patients with Myocardial Infarction in contrast to control groups (6.7% versus 1.3%). It is pertinent to note that the MI subjects have tented arch only in index finger of both the hands. (Table 1 & 2). Contrarily control subjects have tented arch pattern in the index & middle finger. Thus our study presented an interesting fact that the tented arch pattern compared to whorl, loop and arch type proves to be more associated with Myocardial Infarction.
Table 1 Finger print patterns seen on the right hand
|
GROUP |
Total | |||
|
MI Right Hand |
Control Right Hand |
|||
| INDEX | Arch Count% within GROUP |
7 9.3% |
5 6.7% |
12 8.0% |
| Tented Arch Count% within GROUP |
5 6.7% |
1 1.3% |
6 4.0% |
|
| Radial Loop Count% within GROUP |
6 8.0% |
2 2.7% |
8 5.3% |
|
| Ulnar Loop Count% within GROUP |
29 38.7% |
38 50.7% |
67 44.7% |
|
| Whorl Count% within GROUP |
28 37.3% |
29 38.7% |
57 38.0% |
|
| Total Count% within GROUP |
75 100.0% |
75 100.0% |
150 100.0% |
|
Table 2 Finger print patterns seen on the left hand
|
GROUP |
Total | |||
|
MI Left Hand |
Control Left Hand |
|||
| INDEX | Arch Count% within GROUP |
10 13.3% |
6 8.0% |
16 10.7% |
| Tented Arch Count% within GROUP |
5 6.7% |
1 1.3% |
6 4.0% |
|
| Radial Loop Count% within GROUP |
12 16.0% |
1 1.3% |
13 8.7% |
|
| Ulnar Loop Count% within GROUP |
22 29.3% |
43 57.3% |
65 43.3% |
|
| Whorl Count% within GROUP |
26 34.7% |
24 32.0% |
50 33.3% |
|
| Total Count% within GROUP |
75 100.0% |
75 100.0% |
150 100.0% |
|
Rekha and Senthilkumar – Dermatoglyphic patterns in Myocardial Infarction
Discussion
Our study showed an increased frequency of loop pattern in control groups than that of MI group. The percentage of radial loop was decreased in both the categories compared to that of ulnar loop, whereas the observations by Shamsadini et al., (1997) revealed a statistically significant increased frequency of loop pattern in Myocardial Infarcted subjects when compared to control group. Rashad et al., (1975) and Dhall et al., (2000) investigated on these dermatoglyphic patterns and their study revealed a higher frequency of whorl pattern in right thumb, right little finger and left ring fingers of patients with Myocardial Infarction. But our study showed a significant whorl patterns in both thumb and middle finger, right ring finger and in left index finger of the same group. Jalali and Hajian-Tilaki (2002) reported in his subgroup analysis that significant relation between arch types of pattern was made in relation with risk of Myocardial Infarction. Anderson et al., (1981) conducted a study on dermatoglyphic features in association with Myocardial Infarction in Japanese males by using a sample of Caucasian males. It was observed that there were no statistically significant differences in pattern type frequency among Caucasian population between samples of MI and control subjects. Interestingly the present study showed that Tented Arch pattern compared to whorl, loop and arch type proves to be more associated with Myocardial Infarction
Dermatoglyphic patterns form in utero during early gestation and may be influenced by genetic or environmental factors operating at that time. Since cardiac embryogenesis also occurs during early gestation, an analysis of dermatoglyphics in heart diseases might reveal some types which are associated with aberrant dermato- glyphics (Alter and Schulenberg, 1970). Our findings indicated that there is a significant relation between the tented arch type of fingerprint and the risk of MI. Thus dermatoglyphic analysis of subjects can help in early detection of people with suscep- tibility to Myocardial Infarction particularly among those without major risk factors especially among subjects with tented arch type pattern of fingerprint on index finger of both the hands.
Conclusion
From this study it appears that there exist a variation in dermatoglyphic patterns of Myocardial Infarction and it suggests that antenatal factors contribute to the etiology of Myocardial Infarction in humans thereby serving as a screening and early detection tool for the prevention of disease.
References
Alter M, Schulenberg R (1970) Dermatoglyphics in congenital heart disease. Circulation, 41:49-54.
Anderson MW, Haug PJ, Critchfield G (1981) Dermatoglyphic features of Myocardial Infarction Patients. Am J Phys Anthropol, 55:523-527.
Cummins H, Midlo C (1961) Fingerprints, palms and soles: An introduction to Dermatoglyphics. Dover publications, 471th edition. pp1-5.
Dhall U, Rathee SK, Dhall A (2000) Utility Of Finger Prints in Myocardial Infarction Patients. J Anat Soc of India, 49: 1-4.
Jalali F, Hajian-Tilaki KO (2002) Acomparative study of dermatoglyphic patterns with Myocardial Infarction and control group. Acta Medica Iraniaca, 40: 187-191.
Rashad MN (1975) Dermatoglyphic traits in patients with cardiovascular disorders. Am J Phys Anthropol,Vol. 42: 281-283.
Rashad MN, Mi MP, Rhoads G (1978) Dermato- glyphic studies of Myocardial Infarction patients. Hum Hered, 28: 1-6.
Schaumann B, Alter MA (1977) Dermatoglyphics in medical disorders. Psychological Medicine, 7:547-547.
Shamsadini S, Masoomi M, Nejadhosein MA (1997) Relationship between fingerprint dermato- glyphics in association with susceptibility to Myocardial Infarction in man. J Kerman Univ Med Sci, 4: 7-8.
Takashina T, Yorifuji S (1966) Palmar Dermato- glyphics in Heart Disease. JAMA, 197: 689-692.