International Journal of Anatomical Sciences 2013, 4(1):24-26
Research Paper
Variations in the Venous Patterns of the Head and Neck
Sree Lekha D, Sai Sucheethra D, Swayam Jothi Dorai Raj S, Uday Kumar P.
Department of Anatomy, Guntur Medical College, Guntur – 522 004, Andra Pradesh, India.
Key words: venous pattern – venous drainage – head & neck
Abstract: In this study, variations in venous patterns of the head & neck studied in 30 human cadavers were reported.
IVeins are known for their variations than arteries. The anterior facial vein is the chief vein of the face. Since the veins of the head & face are without valves the communication of the anterior facial vein with the ophthalmic vein and also with the infraorbital and buccinator veins are of special clinical importance.(Hollinshead 1961)
Materials and Methods
Venous drainage of face was observed in 30 cadavers. In an adult male cadaver during routine dissection the anterior facial vein was traced.
Observations
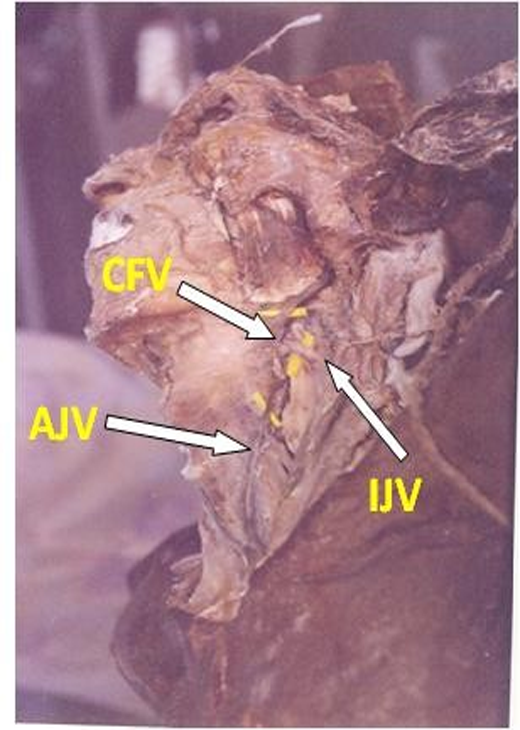
The variation found in one male cadaver was as follows. On the left side four deep facial veins were seen connecting the anterior facial veins with the pterygoid plexus of the veins (Fig.1) The size of the anterior facial vein was average, joined a large anterior division of posterior facial vein to form a large common facial vein. The common facial vein divided into two – one drained into the internal jugular vein and the other division was large and continued as prominent, large anterior jugular vein (Fig.2). The posterior division of retromandibular vein was small and it joined with the posterior auricular vein to form a thin external jugular vein and it soon divided into finer divisions and disappeared over the middle of the strenocleidomastoid muscle (Fig.3) Beyond that existence of external jugular vein could not be made out in the posterior triangle.
|
|
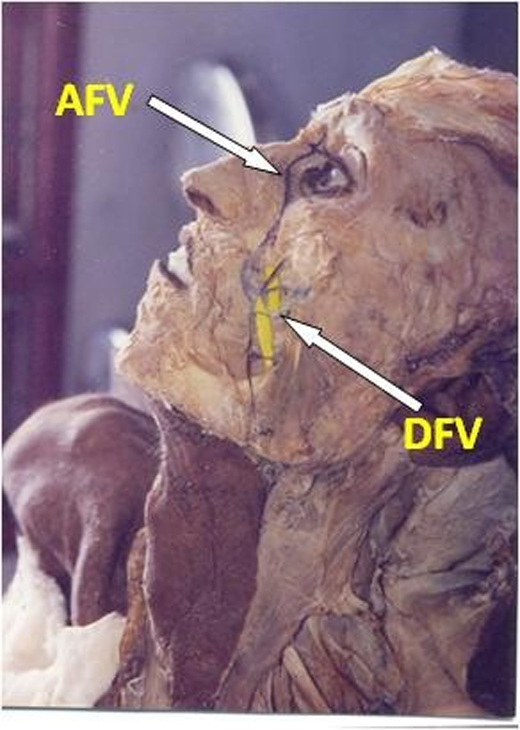
(AFV – Anterior Facial Vein, DFV – Deep Facial Vein)
Fig. 1 On the left side four deep facial veins were seen connecting the anterior facial veins with the pterygoid plexus of the veins
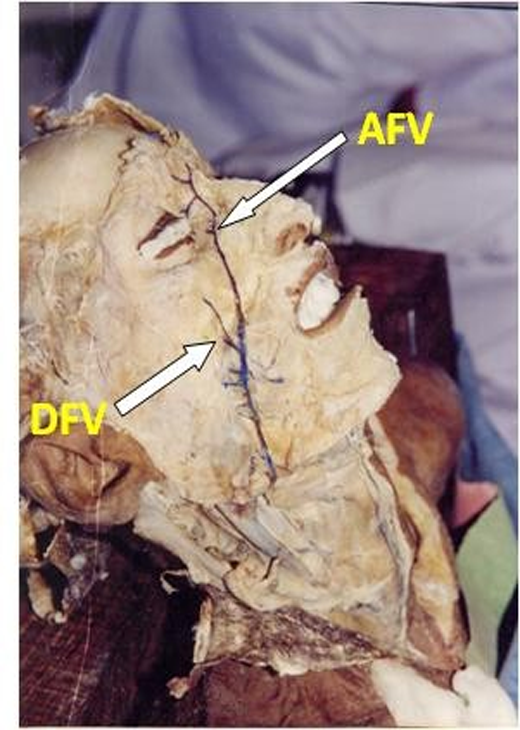
On the right the anterior jugular vein was connected to the pterygoid plexus of veins by four deep facial veins (Fig.4) The course, formation and drainage of other veins of head and neck were normal on the right side.
|
(CFV-Common facial vein, AJV-Anterior jugular vein, IJV- Internal jugular vein)
Fig.2 Common facial vein divided into two – one drained into the internal jugular vein and the other division was large and continued as prominent, large anterior jugular vein

|
(EJV- External jugular vein. IJV- Internal jugular vein)
Fig 3 External jugular vein and it soon divided into finer divisions and disappeared over the middle of the strenocleidomastoid muscle
|
(AFV – anterior facial vein,DFV –Deep facial vein)
Fig. 4 On the right side the anterior jugular vein was connected to the pterygoid plexus of veins by four deep facial veins.
Discussion
Because of the connections of the anterior facial vein it has often been emphasized that infections above the area of the mouth should not be touched from the point of view of attempting to evacuate them for instance. (Pratt 1937; Maes 1937). Roeder (1936) suggested ligation of veins as a prophylactic measure, in order to present spread of infection to the cavernous sinus. Maes (1937) regarded this as of dubious value because once the thrombus has reached the sinus, surgical treatment is of little use because of the development of meningitis. In the present case there were four deep facial veins connecting the anterior facial vein with the pterygoid plexes of veins which are connected to the cavernous sinus.
The anterior jugular vein usually begins in the suprahyoid region through the confluence of various and variable superficial veins or it may arise more laterally from the posterior or common facial veins or parotid veins. In this case it was arising from the common facial vein.
The external jugular vein, begins in the substance of the parotid gland where it is most often formed by the union of the posterior facial and the posterior auricular vein (Brown 1941) or quite variably by a single one or some communications of these and the common facial, internal maxillary or other veins in the parotid region. Close to the parotid gland it received a communication from the internal jugular vein. In the present case the size of the external jugular vein was smaller and faded away forming a plexus at the middle of the sternocleidomastoid muscle.
Conclusion
The case is presented for the clinical significance of variable location of the veins of the face. Since numbers of veins were leading from the danger area of the face to the pterygoid plexus of veins, the danger of spread of infection is much more and this is a precarious situation for cavernous thrombosis to the precipitated
References
Brown S (1941) The external jugular vein in American White and Negroes. Am J Phy Anthropol, 28: 213.
Hollinshead WH, Anatomy for Surgeons, Volume 1: Head & neck. 2nd edition. Harper. Pages 317, 318, 484.
Pratt GH (1937) Furuncle of upper lip. Am J Surg, 36: 118.
Maes U (1937) Infections of the “dangerous area” of the face. Surgery, 2:789.
Roeder CA (1936) The treatment of infections of the face by prophylactic venous destruction. Ann Surg, 104: 1112.